
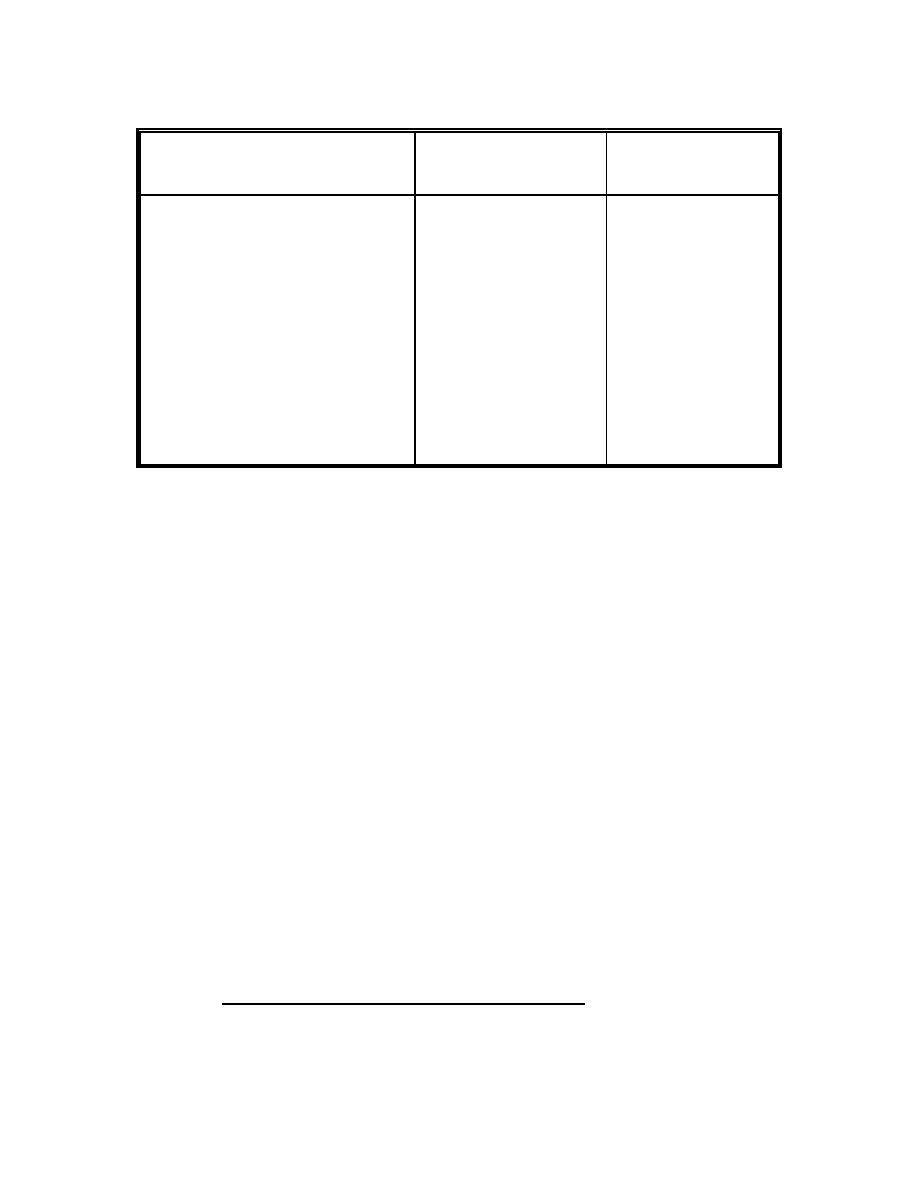
Disease and
Battle Injury
War Period and Location
Noncombat Injury
(percentage)
(percentage)
5
95
Pacific Theater of Operations
Nov 1942 to Aug 1945 (WWII)
23
77
European Theater of Operations
June 1944 to May 1945 (WWII)
17
83
Korean War
July 1950 to July 1953
18.2
81.8
Vietnam War
1 Jan 1969 to 31 Dec 1969
Table 1-1. US Army hospital admissions during selected war periods
1-3.
PREVALENCE OF DISEASE IN PEACETIME
Prevalence of disease in peacetime serves as a baseline against which to estimate
probable wartime incidence and attack rates. Acute respiratory infections often account
for about one-third of the disease admissions among active duty Army personnel.
Normally, the second most frequent cause of admission is nonbattle injury. Diseases of
the digestive system account for about 10 percent of admissions.
Often mild cases of illness are not seen by the medical service, and asymptotic
infections go unreported. This is known as the "iceberg effect."
1-4.
RESPONSIBILITIES FOR HEALTH
a. The Commander and Trained Specialists. The commander of a military
organization is responsible for the health of his command. In the fulfillment of this
responsibility, he is assisted by a staff of trained specialists. The surgeon, who is the
chief medical advisor to the commander, provides technical medical advice and is
responsible for the successful functioning of the medical service within the command.
b. Military Medicine and War
(1) Military medicine part of the machinery of war. Military medicine is an
active part of the machinery of war. Unless military medicine is thoroughly integrated
into military plans and operations, unnecessary costs in manpower and in time loss may
be the price paid to gain objectives.
MD0152
1-3

 Previous Page
Previous Page
