
(d) Follow local standing operating procedure (SOP) for the complete
procedure.
(e) Aspirate air or fluid from the chest cavity. Continue aspiration until
there is no more air or fluid to remove or until over 500 ml of blood or 1000 ml of air
have been removed. A tube thoracostomy (a surgical creation of an opening into the
chest wall) is usually performed when the casualty is evacuated to a treatment facility.
(2)
Perform chest decompression.
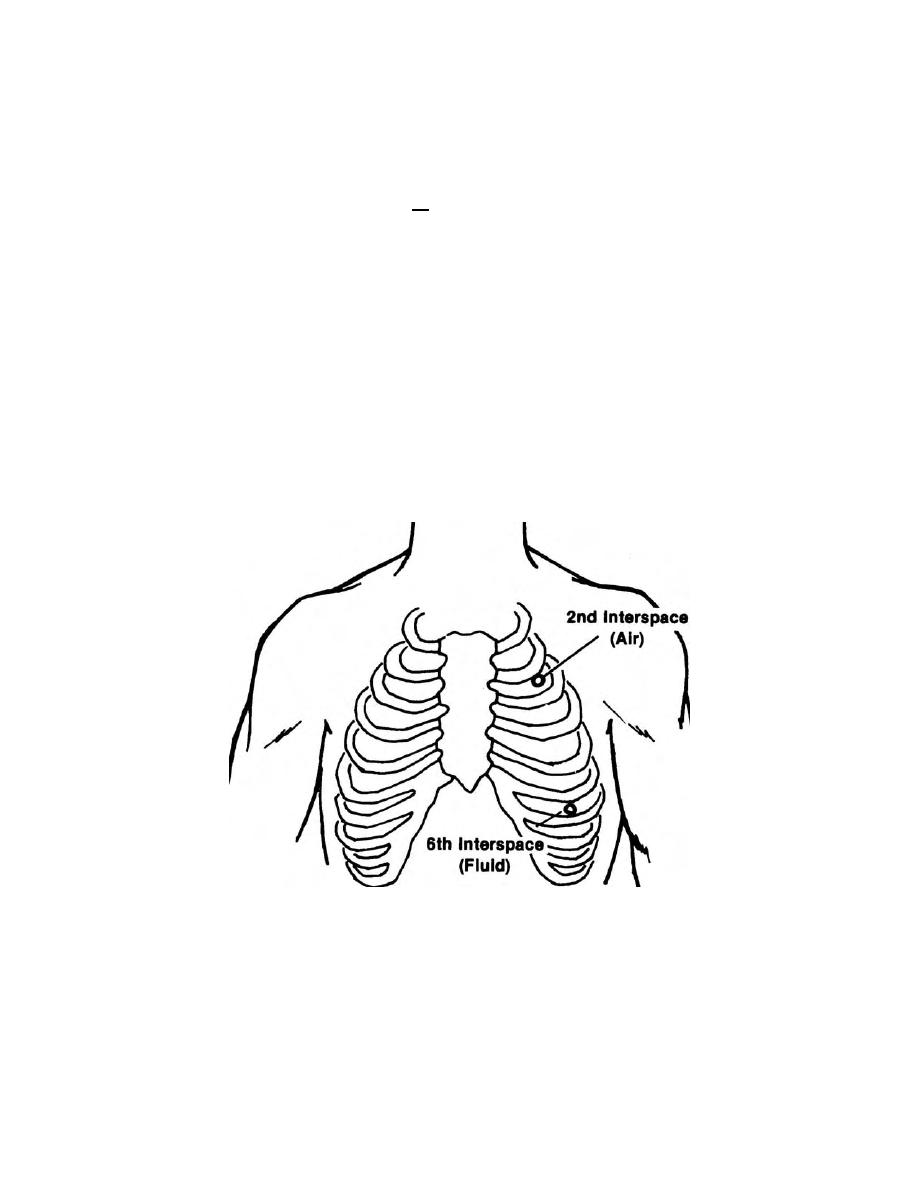
(a) For closed injuries, insert a large bore needle into the second
incostal (ICS) mid-clavicular line (MCL). The plunger rises on its own when under
pressure.
(b) For an open injury, cover the injury with a dressing and periodically
remove the dressing to let air escape.
(3) Perform a tube thoracostomy using the second incostal mid-clavicular
line. This procedure is a must if the casualty is to be air-transported.
Figure 1-5. Needle insertion site for tension pneumothorax.
(4) Give the highest concentration of oxygen possible. Use positive
pressure as needed. The positive pressure may increase tension; however, if
decompression has been accomplished (air removed from the chest cavity), the lungs
may expand.
MD0569
1-15

 Previous Page
Previous Page
