
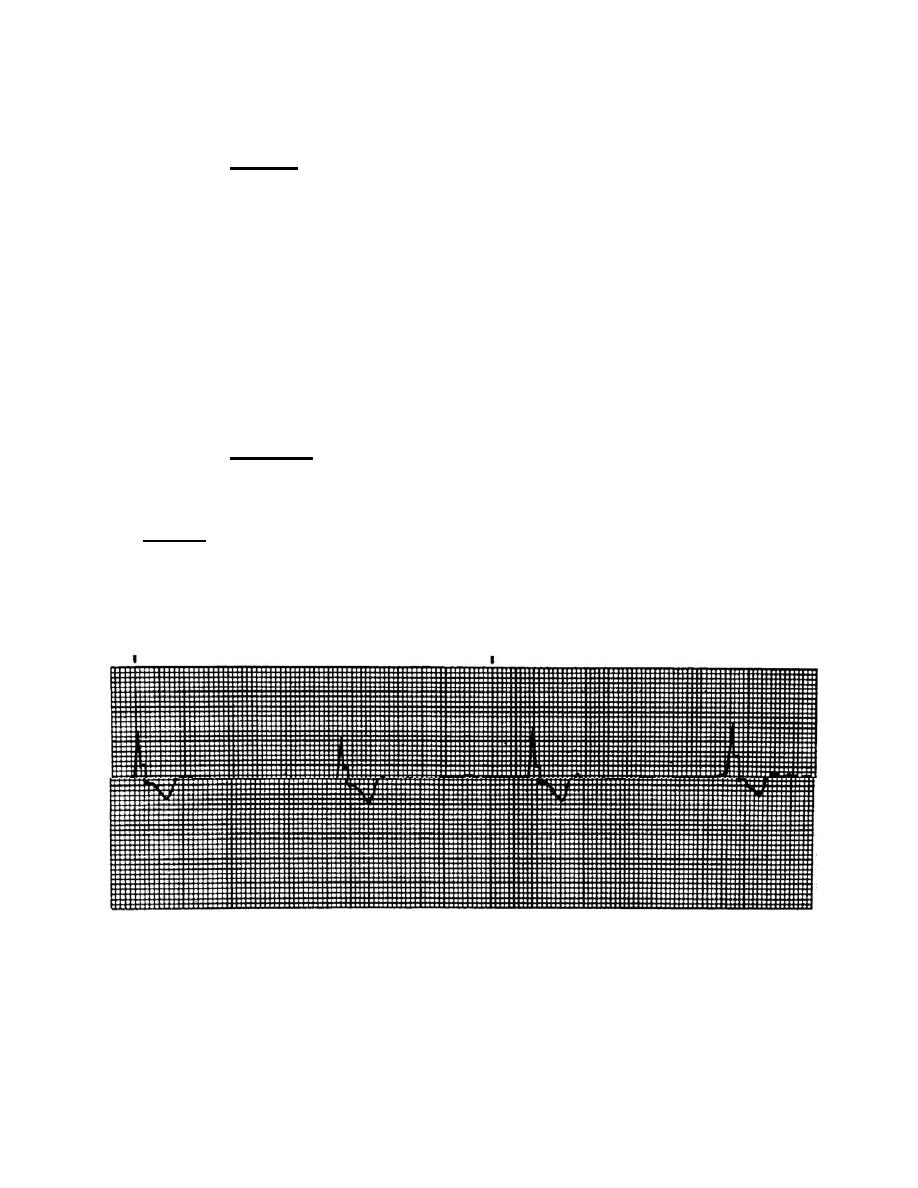
e. Complete Heart Block (Third-Degree).
(1) Analysis. The rhythm is regular with PP and RR intervals constant. The
atrial rate is normal, but the ventrical response rate varies in this way. The junction
focus has a rate of 40 to 60 beats per minute. The ventrical focus has a rate of 20 to 40
beats per minute. P waves are upright and uniform with more P waves than QRS
complexes. There are no PR intervals because the P waves have no relationship to
QRS complexes. Occasionally, a P wave is superimposed on a QRS complex. The
QRS complex is less than 0.12 seconds at the junctional focus and greater than 0.12
seconds at the ventricular focus. Cardiac output may be greatly diminished if the heart
rate is below 35 to 50 beats per minute. Additionally, in third-degree heart block, the
atria and ventricles are no longer synchronized; therefore, the ventricles do not fill
completely before each contraction, causing cardiac output to be even further reduced.
The ventricular rate may be so slow that circulation cannot be maintained and syncope
(congestive heart failure) or angina may occur.
(2) Treatment. Administer atropine sulfate 0.5 mg IV bolus and repeat at
5-minute intervals to try to maintain a heart rate greater than 60 or until the maximum
dose of 2.0 mg is given. If this treatment is ineffective, administer isoproteronal 2 mg in
500 cc D5W IV piggyback until the blood pressure is 80 or the heart rate is greater than
60. NEVER give lidocaine to a casualty with complete heart block. Lidocaine may
increase the threshold of the conduction system and block part of the conduction
pathways. (You must be able to tell the difference between PVCs and complete heart
block.) And, finally, radio a doctor to have a pacemaker ready.
Figure 2-25. Complete heart block.
MD0571
2-27

 Previous Page
Previous Page
