
c. Additional antigenic determinants such as IA, IB, IH, iH, IP1, IP, iP1, ITP1, and
A1Leb are recognized by antibodies with distinct specificities. Thus, although anti-IP1
reacts only with red blood cells having both I and P1 antigens, it is reacting with a
separate IP1 determinant; it is not a mixture of anti-I and anti-P1.
d. At 4C, low-titer (that is, less than 64) auto-anti-I can be demonstrated in the
serum of most individuals. Such auto-anti-I usually has a narrow thermal range and is
not clinically significant. Nevertheless, because it sometimes reacts at room
temperature, it is the most common cause of difficulty in compatibility testing (see
Subcourse MD0846 Lesson 1, Sections II and III). It may agglutinate red blood cells
only weakly at room temperature but unless prewarmed techniques are used,
complement components may become bound to the red blood cells, leading to a false-
positive indirect antiglobulin test at 37C.
e. High-titer auto-anti-I with a wide thermal range is encountered as the
causative antibody of "cold antibody" autoimmune hemolytic anemia.
f. Anti-I can be encountered as an allo-antibody in the serum of individuals of
the very rare i (adult) phenotype.
g. Although anti-i is rarely encountered in routine blood bank investigations, it is
commonly found in the serum of patients with infectious mononucleosis; usually, it is
present as a weak antibody reacting only at 4C. On rare occasions, it may be present
to high titer and be the cause of "cold antibody" autoimmune hemolytic anemia. Helpful
hints in testing I system antibodies are as follows:
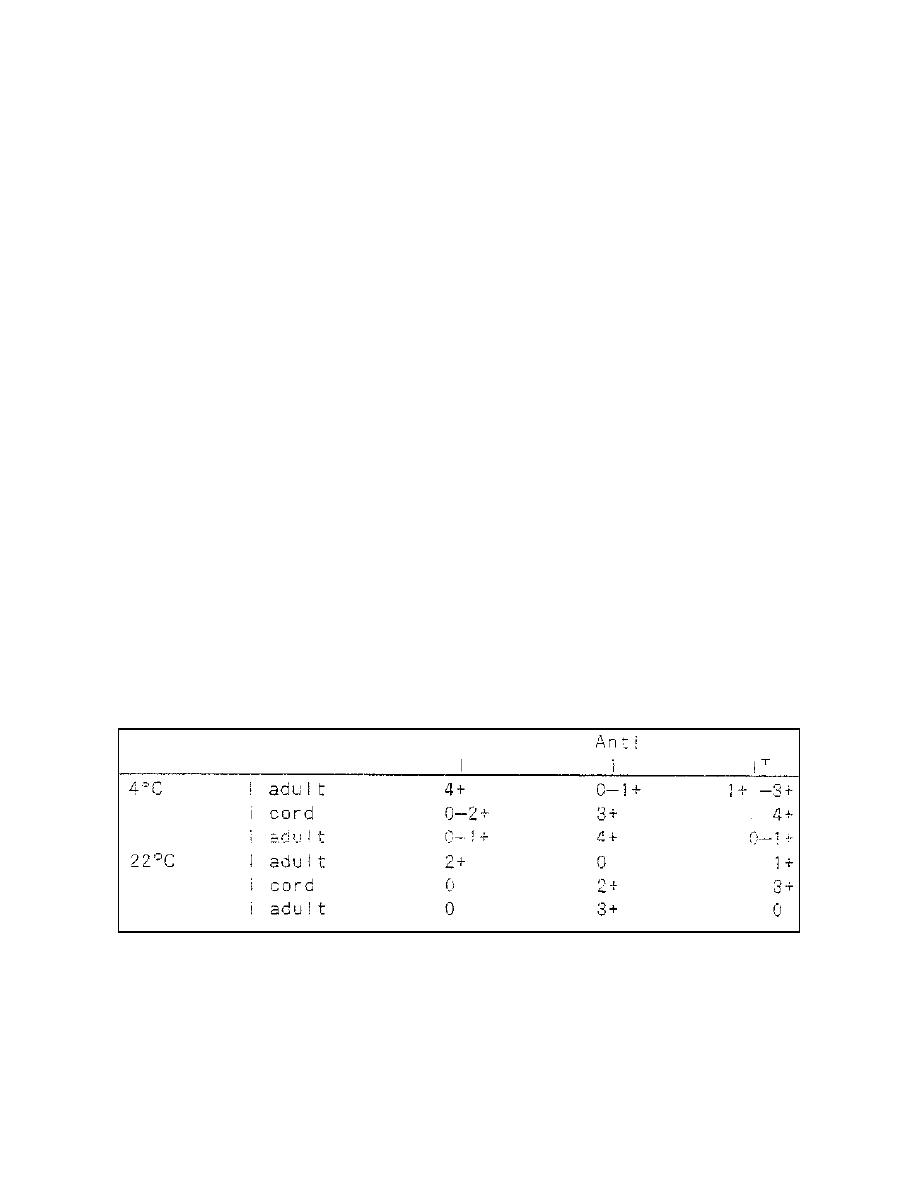
(1) Strong examples of the antibodies may not show the clear-cut
differences shown in Table 2-17. Titration studies at different temperatures to
determine the specificity may be necessary.
Table 2-17. Some examples illustrating the serologic behavior of I system antibodies
(saline cell suspensions).
MD0845
2-49

 Previous Page
Previous Page
