
(2) Fetal distress may be indicated by FHT's, between contractions that are
consistently abnormal. Any variations should be reported immediately.
(3) The FHTs should be checked and recorded on admission, every 15
minutes during the first stage of labor, every 5 minutes during the second stage of labor,
and immediately after rupture of membranes. This helps to identify the location of the
prolapsed cord.
NOTE:
The prolapsed cord is referred to as the umbilical cord that protrudes beside
or ahead of the presenting part of the fetus. Pressure of the presenting part
on the umbilical cord can endanger fetal circulation.
(4) Fetal monitoring continued. According to the National Institute of Health
(NIH), electronic fetal monitoring of the fetus is not necessary during normal labor.
However, if either the mother or fetus is considered at risk, a more precise
measurement of fetal response is indicated.
(5) Candidates for continuous fetal monitoring includes a patient with a
multiple pregnancy, a patient with obstetric complications, a patient receiving oxytocin
infusions, any high risk patient, a patient with meconium stained amniotic fluid, or any
patient whose pregnancy is not progressing normally.
(6) Most medical facilities are using continuous fetal monitoring during labor.
Alternative birth centers often use intermittent monitoring.
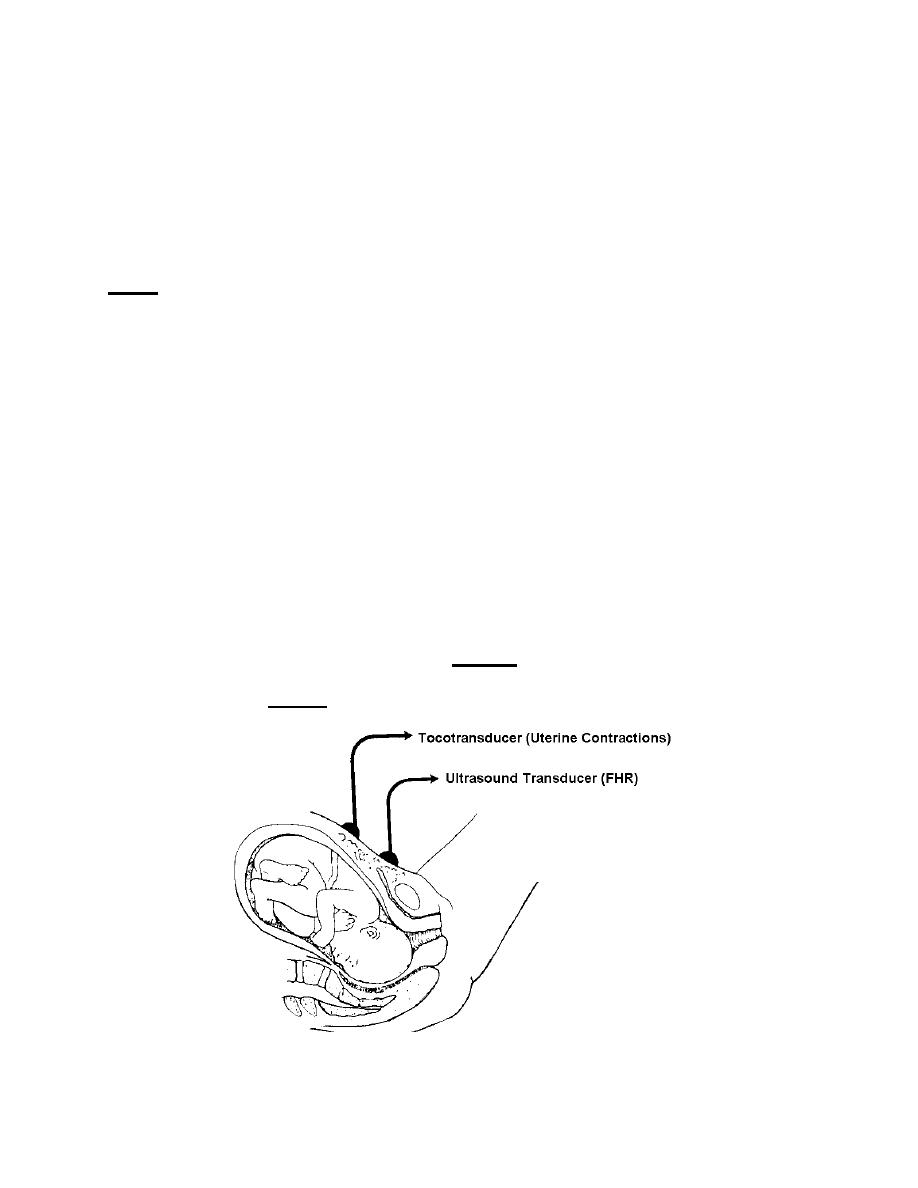
(7) Methods of fetal monitoring (see figures. 2-4 and 2-5). A transducer is
placed on the abdomen over the uterus for external monitoring. An electrode is
attached to the presenting part of the fetus, but NOT placed on the sutures, fontanels,
face, or scrotum for internal monitoring.
Figure 2-4. External fetal monitoring,
MD0922
2-11

 Previous Page
Previous Page
