
(5) The surgeon places the forefinger of one hand into the rectum via the
finger cot in the O'Connor drape and pushes the prostate gland forward. With the
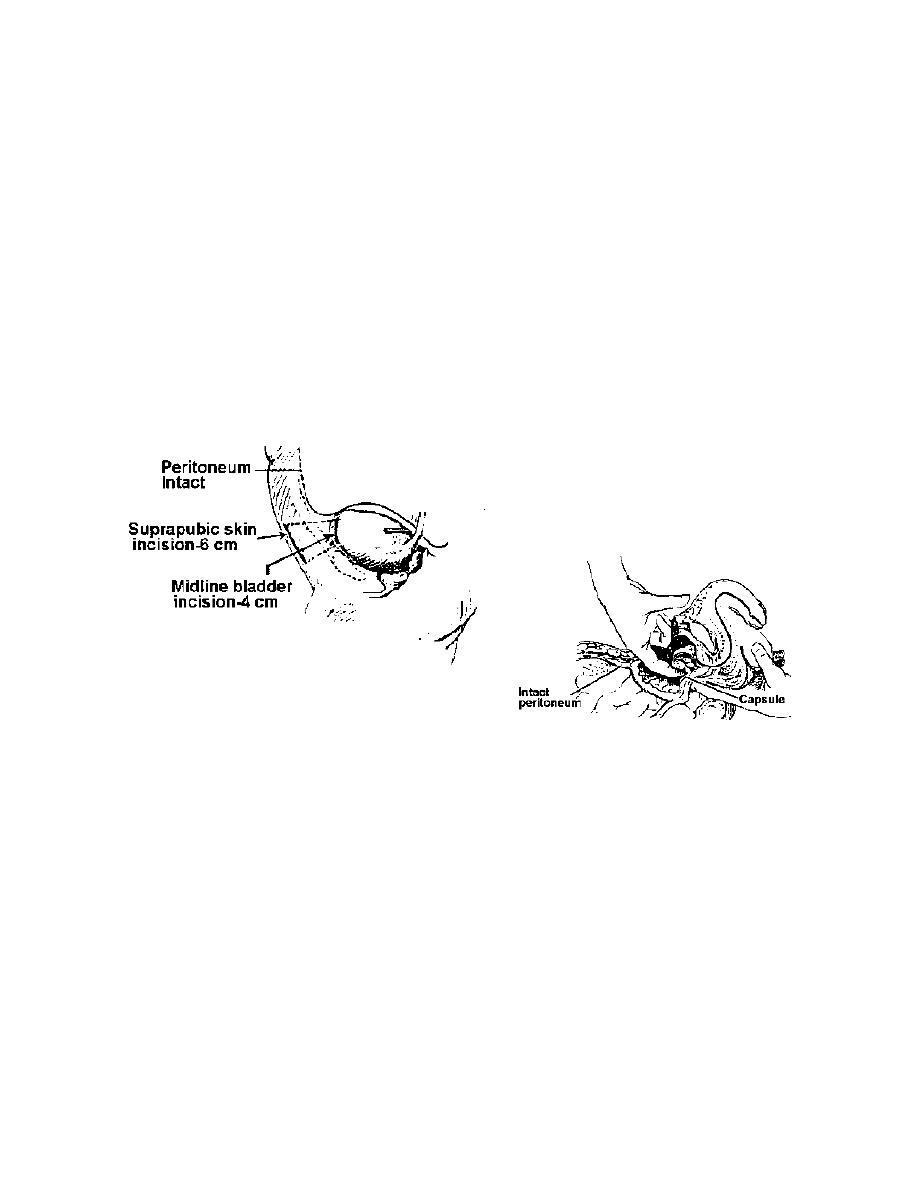
forefinger of the operating hand, the lobes of the gland are enucleated from the capsule
(see figure 3-9). Bleeding is controlled with hemostats and ligatures, sutures, or
electrocoagulation. Long forceps, half-length sutures, and long needle holders are
required for placing sutures.
(6) Following removal of the prostate and control of bleeding, a hemostatic
catheter with an inflatable bag--Foley 24 Fr with a 30-ml bag may be placed in the
fossa; the balloon is adjusted under direct vision and inflated, using sterile water in a
30-ml syringe with an adapter. A hemostatic cone of Gelfoam may be used if preferred.
(7) The bladder is closed as for suprapubic cystostomy with a Malecot
catheter in place. One or two wide Penrose drains may be placed in the prevesical
space of Retzius. The wound is closed in layers and dressed.
Figure 3-9. Enucleation of prostate by suprapubic approach.
3-29. RETROPUBIC PROSTATECTOMY.
a. General. This operation involves enucleation of the prostatic hypertrophied
lobes directly through a capsular incision in the upper surface of the prostate rather than
through the bladder.
b. Operative Procedure. See Figure 3-9.
(1) Through a vertical or transverse suprapubic incision, the abdominal wall
is opened to expose the space of Retzius. The bladder is not directly opened. The
precystic fat is extracted using long, smooth tissue forceps. Large vessels are ligated,
using 18-inch transfixion sutures of chromic gut number 0 threaded on small Mayo
needles.
MD0928
3-30

 Previous Page
Previous Page
