
a.
Facts Concerning Respiratory Distress.
(1)
Respiratory distress is caused by laryngospasms (a complication
that may happen after the patient's endotracheal tube is removed by the anesthetist or
anesthesiologist), by aspiration of vomitus, or by preoperative medications. Some
preoperative medications can depress respirations, especially morphine.
(2)
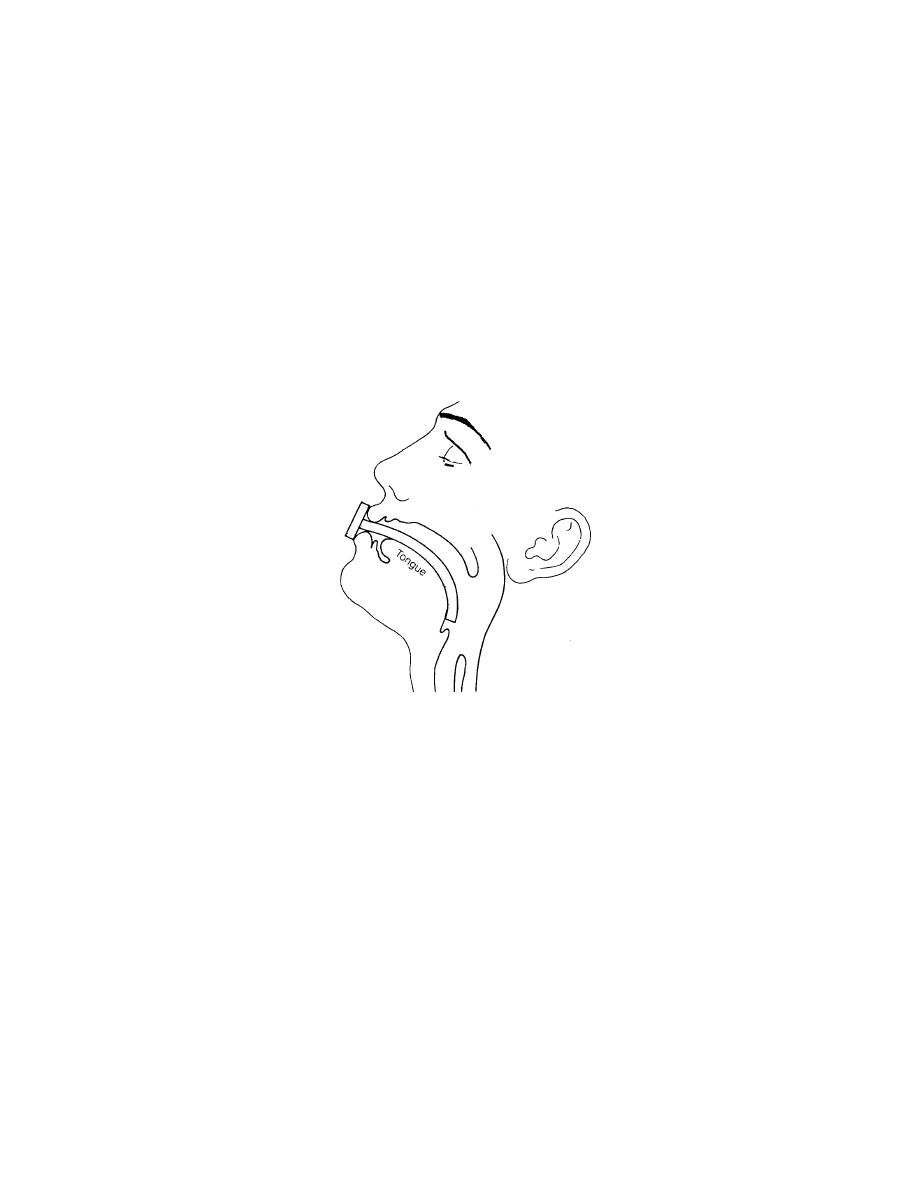
If the patient's breathing is obstructed because his tongue has fallen
back and has obstructed the nasopharynx, the lower jaw is pulled forward and an
oropharyngeal airway is inserted (see Figure 3-2).
(3)
The airway is left in place until the patient is conscious. The airway
prevents the tongue of the unconscious patient from blocking the air passages.
Figure 3-2. An oropharyngeal airway in place.
b.
Nursing Implications to Prevent Respiratory Distress.
(1)
Monitory respiratory status as ordered.
(2)
Report labored and shallow or rapid respirations to the Charge
Nurse.
(3)
Maintain patent airway either with oropharyngeal airway in place or
removed.
(4)
Suction the patient via nose and/or orally as ordered.
(5)
Maintain the patient's position to facilitate lung expansion, usually the
Fowler's position (see Figure 3-3).
MD0915
3-5

 Previous Page
Previous Page
