
e. Fluid Resuscitation Algorithm.
(1) Superficial wounds. More than 50 percent of injured soldiers have only
superficial wounds. These soldiers require no immediate intravenous fluids, but oral
fluids should be encouraged.
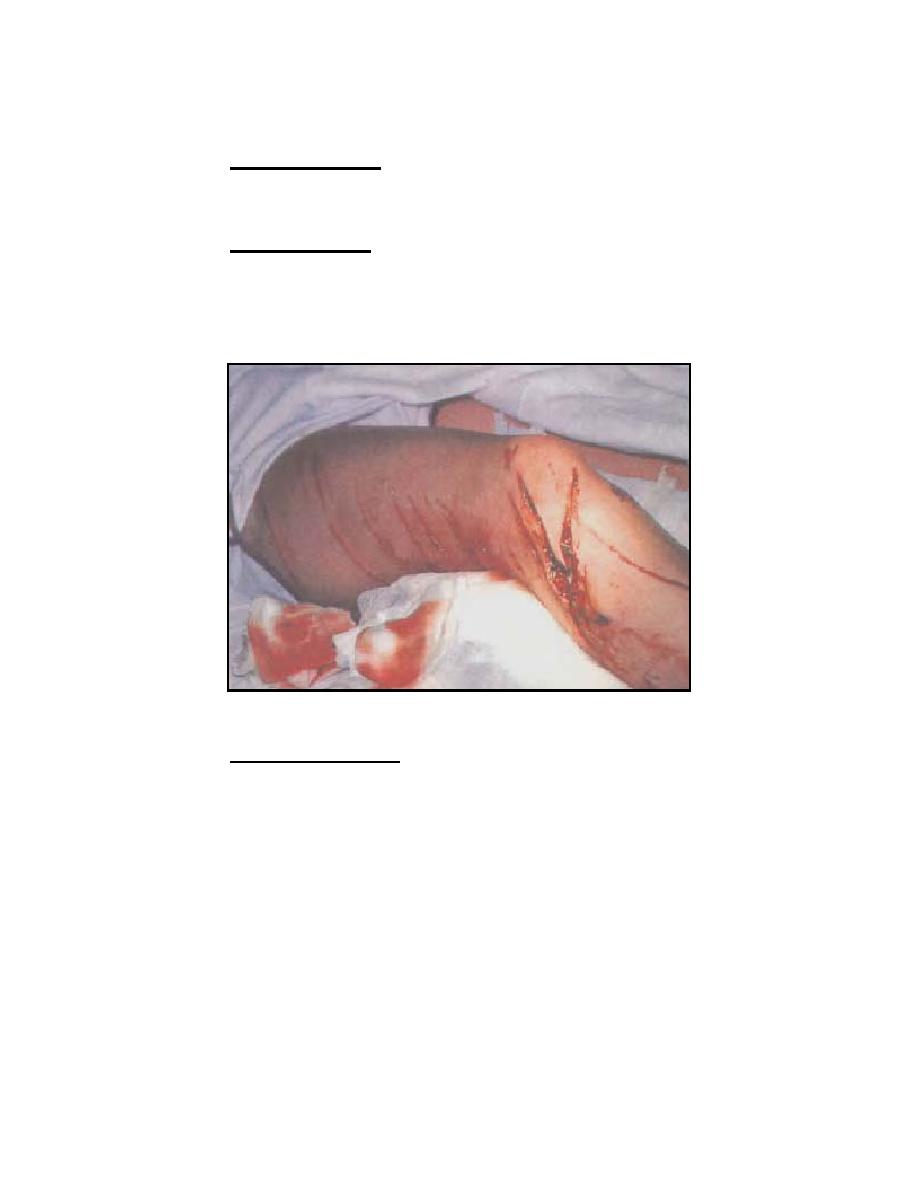
(2) Significant wound. Any significant extremity (arm or leg) or truncal
(neck, chest, abdomen, or pelvis) wound, with or without obvious blood loss or
hypotension, may require an IV (see figure 1-2). If the casualty is coherent and has a
palpable radial pulse, blood loss has likely stopped. Initiate a saline lock, hold fluids,
and re-evaluate as frequently as the situation will allow. If the casualty is not
nauseated, have him sip small quantities of water to assist hydration.
Figure 1-2. Significant wound to the leg.
(3) Significant blood loss. For significant blood loss from any wound where
the soldier has no palpable radial pulse or is not coherent, perform the following.
(a) STOP THE BLEEDING by all means at your disposal (tourniquet,
direct pressure, pressure dressing, hemostatic dressing, hemostatic powder, or other
means). Many of these hypotensive casualties suffer from truncal injuries which are
unaffected by these resuscitative measures (casualty may have lost as much as 1,500
ml of blood [about 30 percent of their circulating volume]).
(b) Once hemorrhage has been controlled to the extent possible,
initiate IV access and administer 500 ml of Hextend. If the mental status improves and
the radial pulse returns, maintain a saline lock and hold fluids. If there is no response
observed within 30 minutes, administer an additional 500 ml of Hextend and monitor
the casualty's vital signs. If no response is seen after 1,000 ml of Hextend has been
administered, you may need to consider rationing your resources and turning your
attention to more salvageable casualties.
MD0553
1-6

 Previous Page
Previous Page
