
8-22. WOUND DRAINS
a. Inserting Drains. The use of drains, tubes, and suction devices at the wound
site is often necessary to promote healing. A drain or tube is inserted into or near a wound
after the surgical procedure is completed. One end of a tube or drain is placed in or near
the incision when it is anticipated that fluid will collect in the closed area and delay healing.
The other tube end is passed through the incision or through a separate opening called a
stab wound. Tubes that are to be connected to suction or have a built-in reservoir are
sutured to the skin. It is important that you know the type of drain or tube in use so that
patency and placement can be accurately assessed.
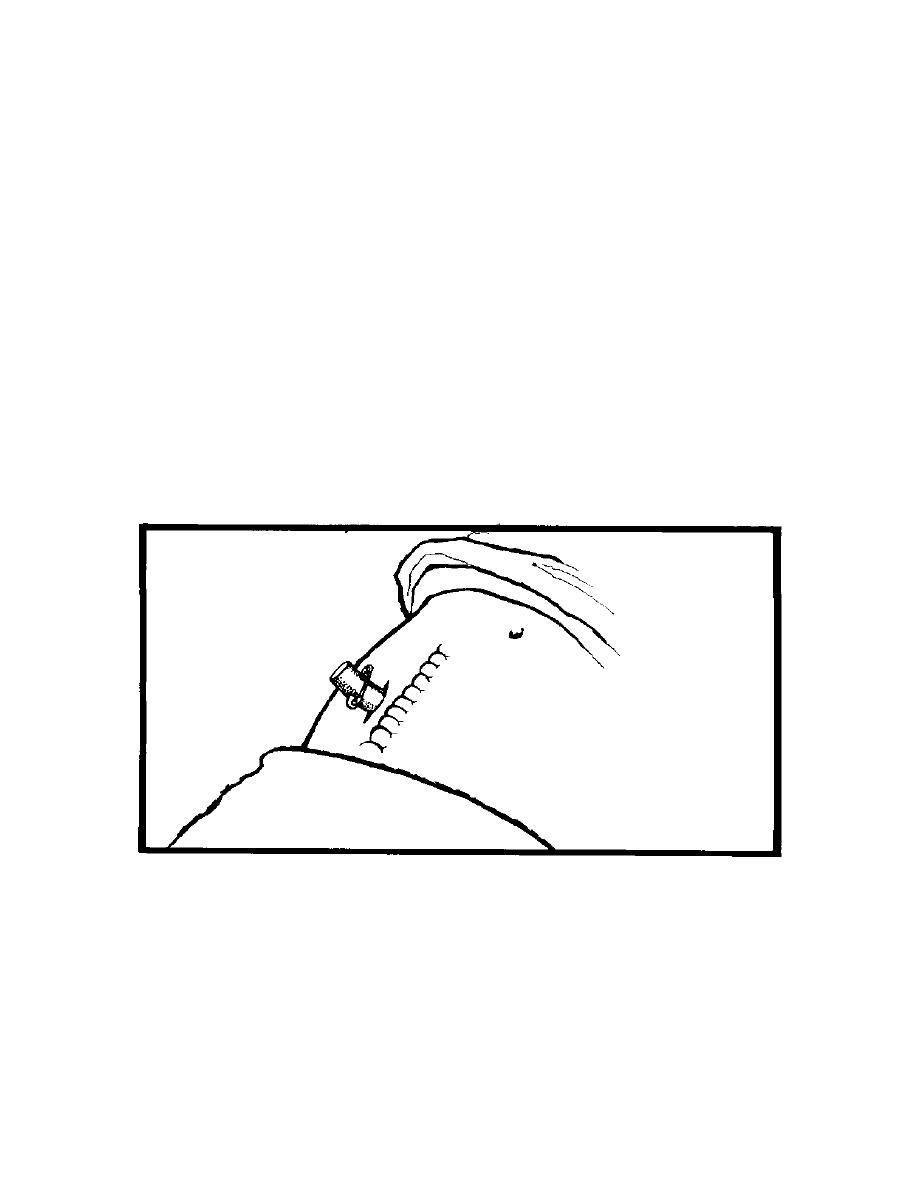
b. Penrose Drain (figure 8-6). This is the most commonly used drain. It is made
of flexible, soft rubber and causes little tissue reaction. It acts by drawing any pus or fluid
along its surfaces through the incision or through a stab wound adjacent to the main
incision. It has a large safety pin outside the wound to maintain its position. To facilitate
drainage and healing of tissues from the inside to the outside, the tube is often pulled out
and shortened 1 to 2 inches each day until it falls out. The safety pin should be placed in
its new position prior to cutting the drain. Advance the drain with a dressing forceps or
hemostat, use surgical scissors to cut excess drain.
Figure 8-6. Penrose drain.
c. Jackson-Pratt/Hemovac Closed Suction Device (figure 8-7). Tubes are
connected to suction or there is a built-in reservoir to maintain constant low suction. In the
operating room, the surgeon places the perforated drainage tubing in the desired area,
makes a stab wound, then draws the excess tubing through the wound creating a tightly
sealed porthole. The tubing is then attached via an adaptor to the suction device. To
establish negative pressure, compress the device and place the plug in the air hole.
MD0906
8-28

 Previous Page
Previous Page
