
(6)
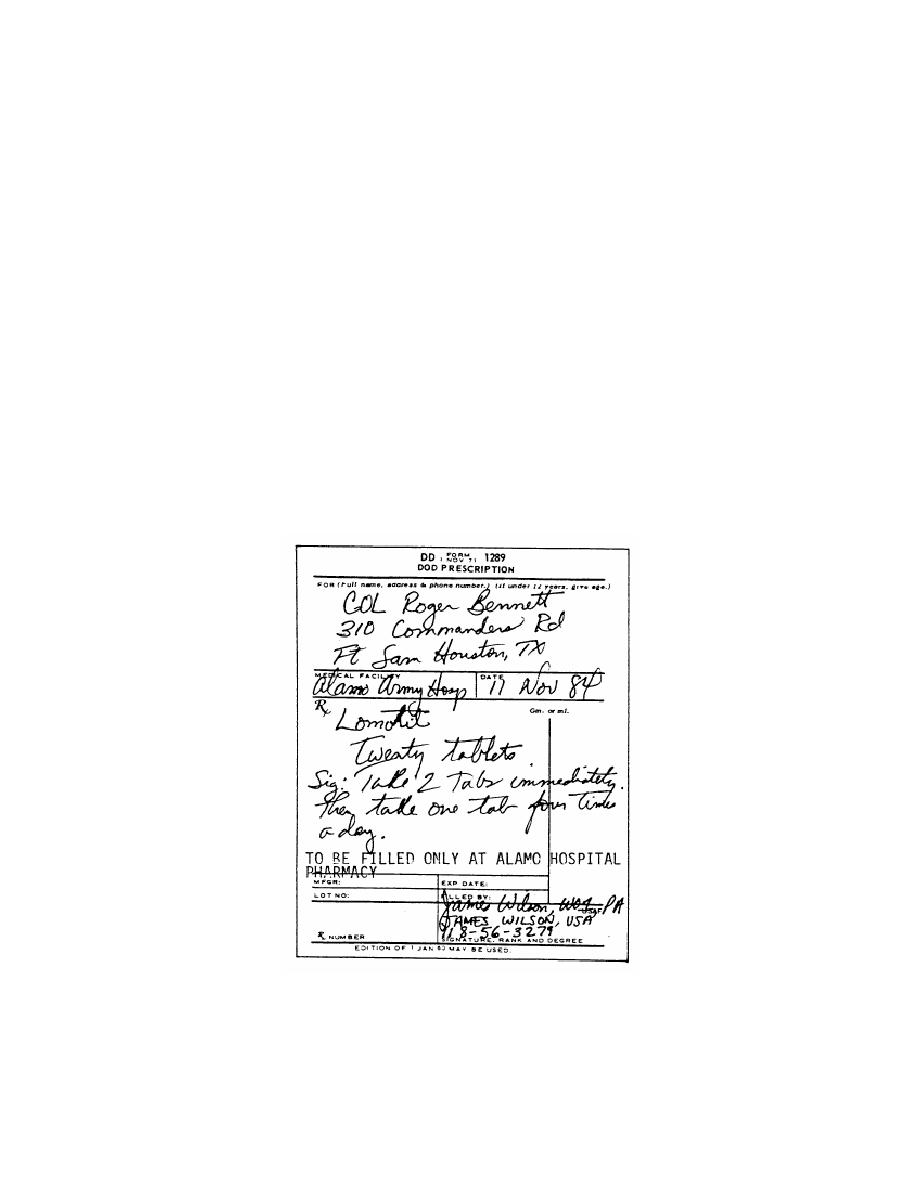
The amount of medication to be dispensed.
(7)
The directions to the patient.
(8)
The refill instructions.
(9) The statement "TO BE FILLED ONLY AT (name of local medical
treatment facility) PHARMACY"--if the prescription was written by a nurse clinician,
graduate physician assistant, physical therapist, or AMOSIST.
(10) The signature of the prescriber--signed in ink on the day the prescription
was written.
(11) The rank and the degree of the prescriber.
d. Information Required on the Prescription Form for a Controlled
Substance. The following information is required on the prescription form for a
controlled substance in order for it to be filled by the pharmacy service of an Army
medical treatment facility. (See figure 3-3.)
Figure 3-3. Prescription for a controlled substance.
MD0810
3-6


 Previous Page
Previous Page
