
b. If your check shows that the casualty is breathing, asses the rate and quality
of breathing. Just because a casualty is breathing does not ensure that the depth of
breathing or the rate are adequate to support life. (If the casualty is breathing 4 times
per minute, he is technically breathing; but this rate is not adequate to sustain the
casualty's life). If the casualty has adequate breathing, consider inserting an airway
adjunct to help control and protect the casualty's airway. If available, oxygen should be
administered at this time. Continue to examine the casualty for injuries while
maintaining his airway. Check on his breathing periodically. Reopen the airway and
perform rescue breathing should the casualty stop breathing.
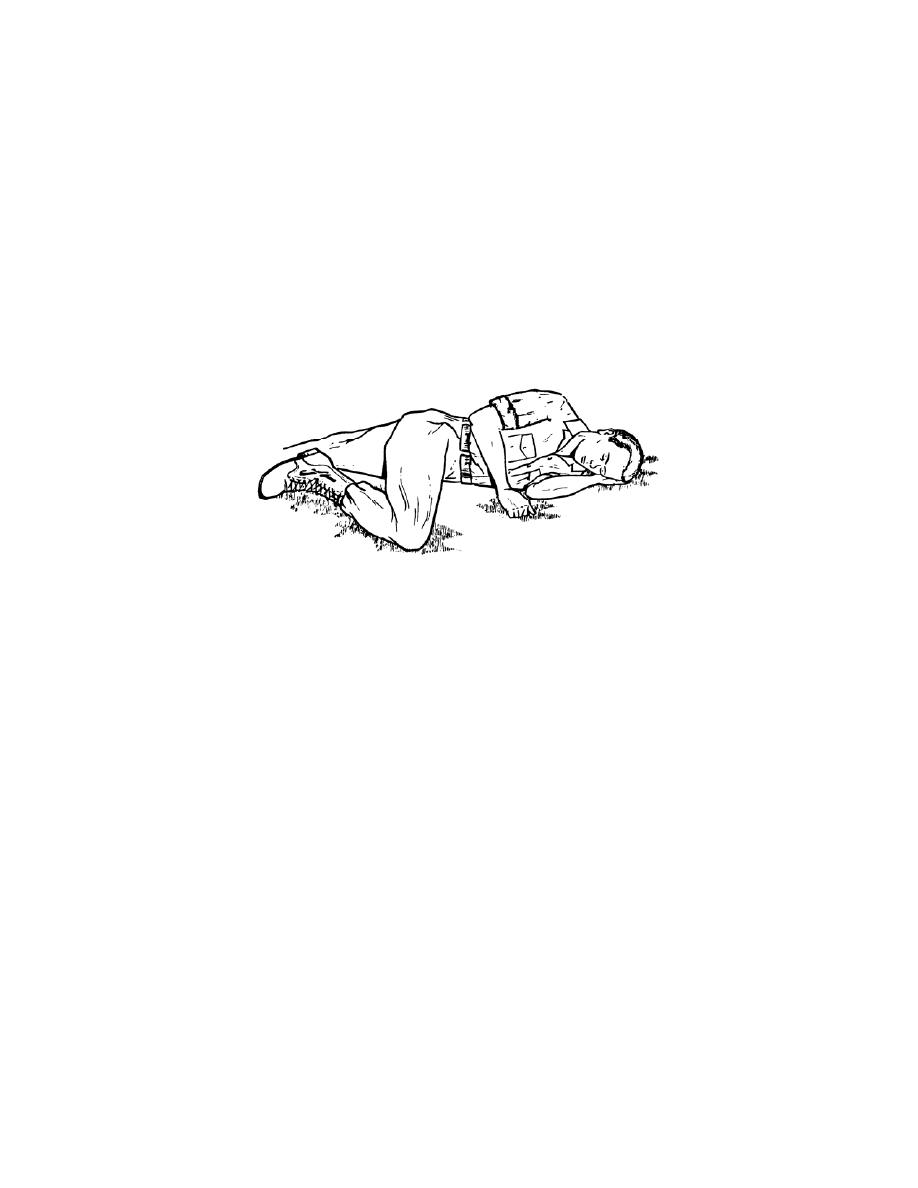
(1) If the casualty regains consciousness, place him in the left lateral
recumbent position (figure 3-5) if no other injuries are present.
Figure 3-5. Unconscious casualty in the left lateral recumbent position.
(2) If the casualty is unconscious and you have an oropharyngeal airway
(OPA or J-tube) available, you can insert the airway to prevent the casualty's airway
from being blocked by his tongue. Remove the airway when the casualty begins to
regain consciousness.
(a) Make sure that you insert the correct size of airway. Place the
oropharyngeal airway along the outside of the casualty's jaw. The airway should reach
from the bottom tip of his ear to the corner of his mouth.
(b) Open the casualty's mouth. If you have difficulty in opening his
mouth, place your crossed thumb and index finger on the casualty's upper and lower
teeth near a corner of his mouth and push until his teeth separate and his mouth opens.
(c) Place the tip end (not the flanged end) of the oropharyngeal airway
into the casualty's mouth so that the tip points toward the roof of the casualty's mouth.
(d) Slide the airway along the natural curvature of the tongue.
MD0532
3-9

 Previous Page
Previous Page
