
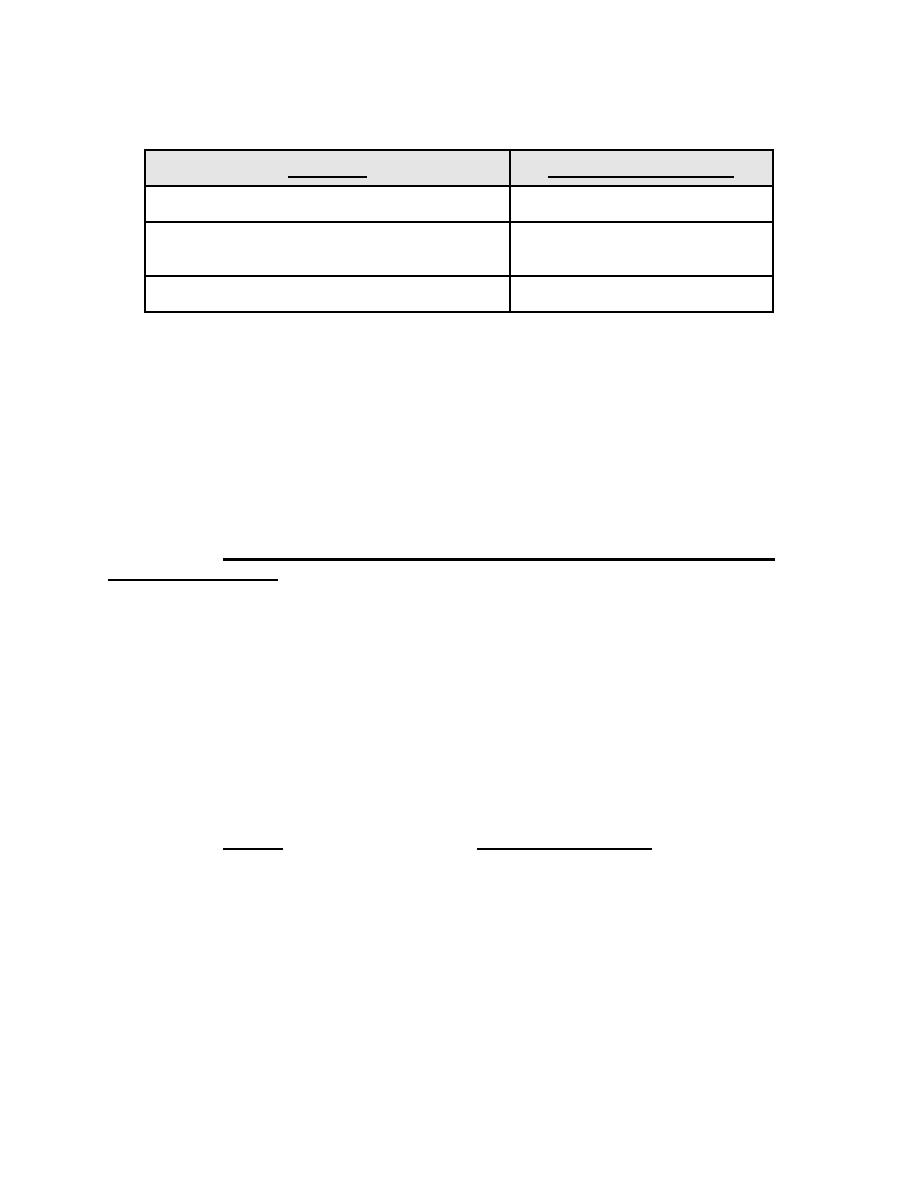
Treatment goals:
Category
LDL-Cholesterol Goal
No atherosclerosis & < 2 risk factors
<160 mg/dl
No atherosclerosis & 2 or more risk factors
<130 mg/dl
Existing atherosclerosis
<100 mg/dl
a. Diet and Exercise. Diet and exercise are considered lifestyle modifications
which may lower cholesterol levels to goal. Diet changes reduce intake of cholesterol
and fat, especially saturated fat. Exercise may involve aerobic exercise for at least 20-
30 minutes, 3-5 times weekly. Whether a patient is on medication to lower their
cholesterol or not, diet and exercise should always be a part of the treatment regimen.
b. Drug therapy Medications are often prescribed for hyperlipidemia when diet
and exercise fail to normalize LDL levels. Agents may prevent cholesterol synthesis or
promote the breakdown of internal cholesterol.
(1) Statins - also called HMG CoA (hydro-methylglutaryl Coenzyme A)
Reductase Inhibitors. HMG CoA is needed to produce mevalonic acid in the body,
which is used to produce many products, among them cholesterol. As cholesterol
synthesis is inhibited, LDL receptor site production is increased to draw cholesterol from
serum. All of the statins work the same but may differ in potency (degree to which they
decrease cholesterol levels). The more potent statins may significantly reduce
triglycerides as well as LDL; some agents may increase HDL (this is good!). Because
our liver makes most of our cholesterol at night, these agents work best when
administered at bedtime. The most common side effects include muscle aches and
weakness, diarrhea, constipation, and headache. Generalized muscle aches (over the
entire body) must be reported immediately as this may indicate a more serious
condition. Common statins include cerivastatin (Baycol), simvastatin (Zocor),
atorvastatin (Lipitor), and pravastatin (Pravachol).
(2) Resins. Resins, also known as bile acid sequestrants, bind to bile acids
in the GI tract and cause us to break down our internally produced cholesterol and thus
lowering our cholesterol levels. Resins may increase triglyceride levels so must be
used with caution in patients that have high triglycerides. Resins are very effective,
however patients express poor compliance with these agents due to the side effects of
heatburn, nausea, flatulence, constipation; dosing regimens; and significant drug-drug
interactions. Resins are positively charged and many medications that carry a negative
charge will bind with them. Medications such as digoxin, thiazide diuretics,
betablockers, warfarin, thyroxine, and fat soluble vitamins (A, D, K, and folic acid)
should not be taken after these agents. If a patient is prescribed a resin, he/she should
take other medications 2 hours before or 4 hours after the resin. These agents are in
MD0806
3-10

 Previous Page
Previous Page
