
NOTE:
If the patient has been transfused with red blood cells in the preceding 4
weeks or thereabouts, autoabsorption should not be performed because the
antigens on the transfused cells may adsorb a developing isoantibody of
clinical significance.
g. Specific Procedures.
(1) To diagnose anti-A1, anti-H, or anti-I, test subject's serum against
carefully selected cells.
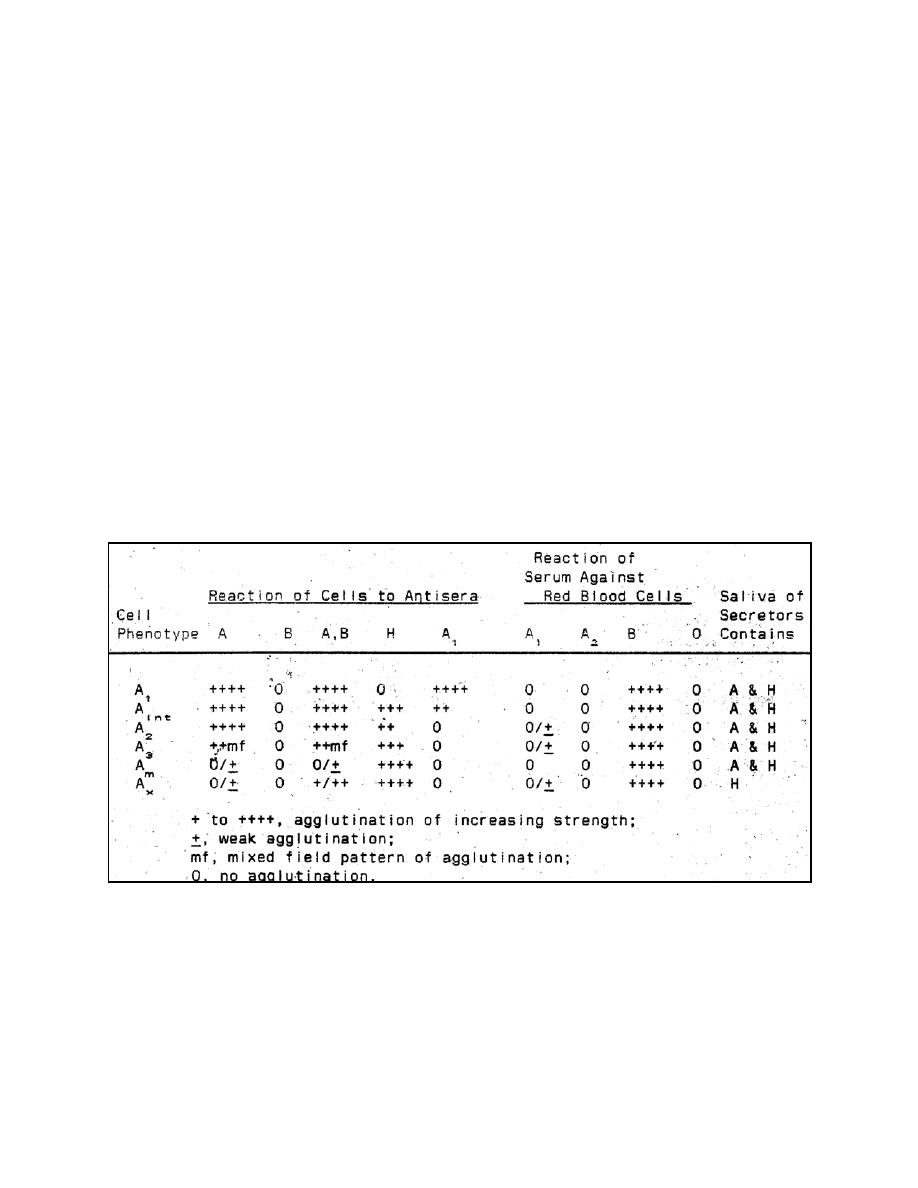
(2) To delineate weak examples of A or B, whether genetic or acquired, a
number of procedures may have to be used. Table 2-7 shows serologic characteristics
of several variant A phenotypes that may be encountered. To diagnose rarer A and B
phenotypes, see Race and Sanger.
(a) Test cells with many different samples of anti-A and anti-B,
including those from subjects whose antibodies have been stimulated by injection of A
or B substances.
(b) Perform anti-A and anti-B testing with incubation at 18C or 4C.
NOTE: The occurrence of anti-A1, is variable in these phenotypes. Ax persons
frequently have anti-A1; A3 persons usually do not, but a few A3 serums with Anti-A1,
have been found. Anti-A1 is more common in A2B serum than in A2 serum.
Table 2-7. Serologic reactions of A phenotypes. (Adapted from Race and Sanger)
MD0845
2-22

 Previous Page
Previous Page
