
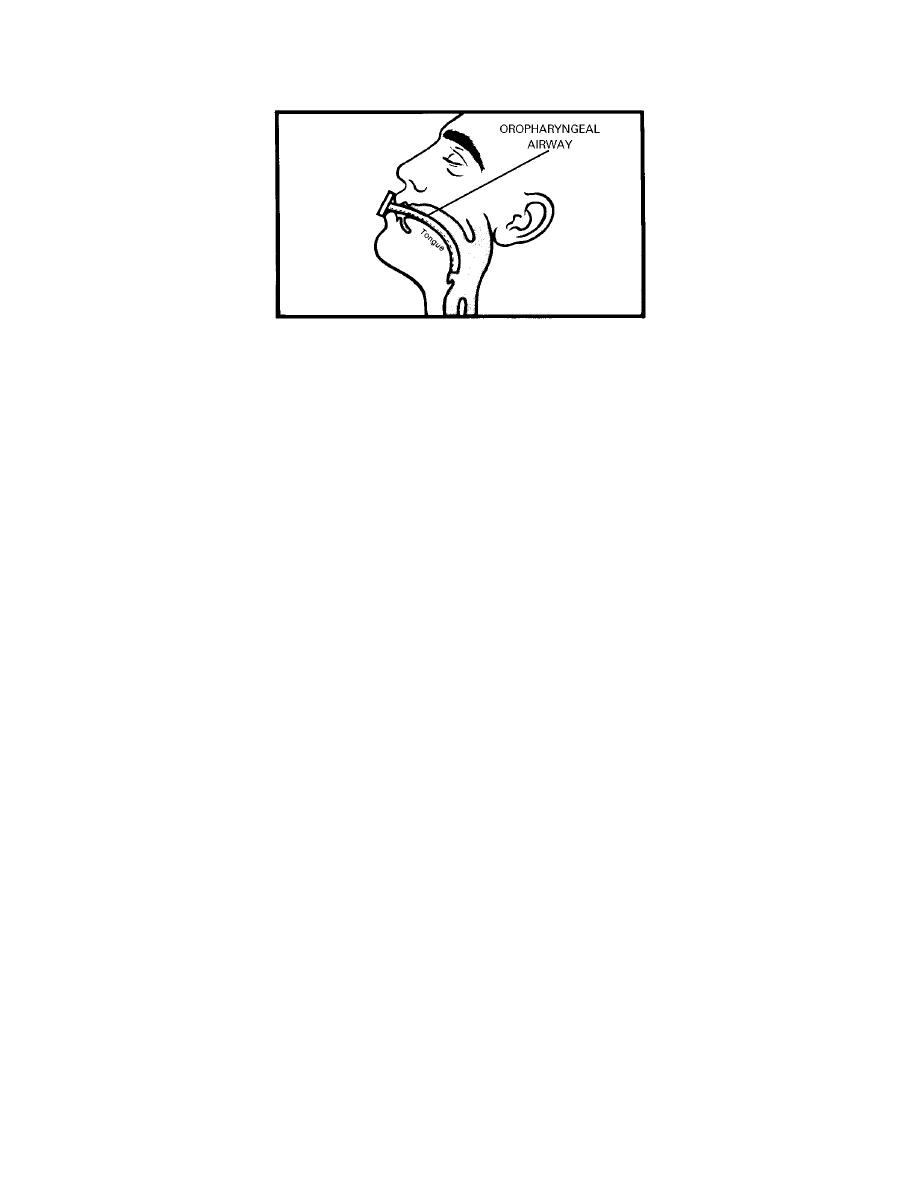
Figure 8-4. Oropharyngeal airway.
(2) Swallowing and cough reflexes are diminished by the effects of anesthesia
and secretions are retained. To prevent aspiration, vomitus or secretions should be
removed promptly by suction.
(3) Ineffective airway clearance may be related to the effects of anesthesia
and drugs that were administered before and during surgery. If possible, an unconscious
or semiconscious patient should be placed in a position that allows fluids to drain from the
mouth.
b. After removal of the endotracheal tube by the anesthesiologist or anesthetist,
an oropharyngeal airway is inserted to prevent the tongue from obstructing the passage of
air during recovery from anesthesia. The airway is left in place until the patient is
conscious.
8-12. PREVENTION OF RESPIRATORY DISTRESS
a. Monitor respiratory status as frequently as prescribed. Respiratory function is
assessed by monitoring the patient's respiratory rate, rhythm, and depth, and by observing
skin color. The following observations indicate ineffective ventilation:
(1)
Restlessness and apprehension.
(2)
Unequal chest expansion with use of accessory muscles.
(3)
Shallow, noisy respirations.
(4)
Cyanosis.
(5)
Rapid pulse rate.
b. Report labored respirations to supervisor.
c. Report shallow, rapid respirations to the supervisor.
MD0906
8-18

 Previous Page
Previous Page
