
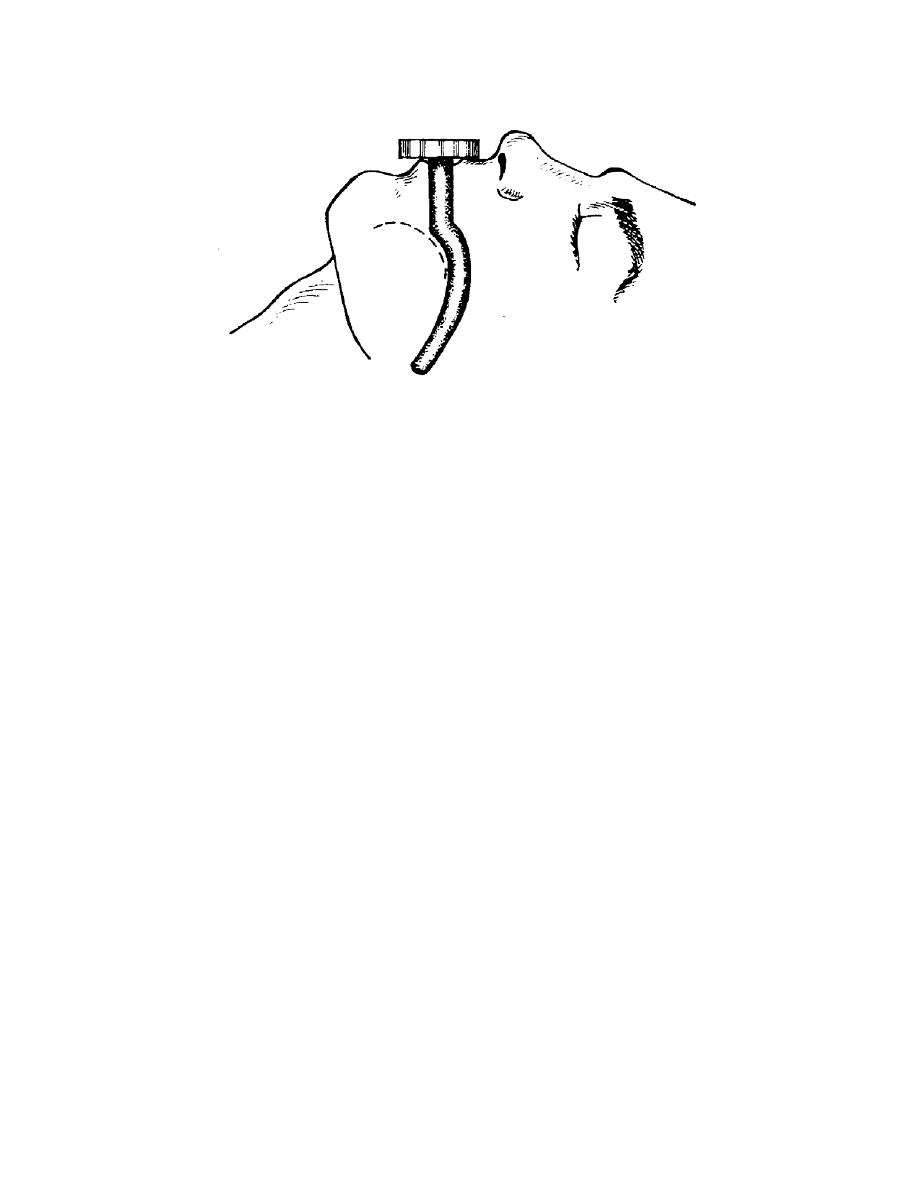
Figure 2-8. J-tube in place.
e. Remove Oropharyngeal Airway, If Needed. When the patient starts to
regain consciousness or gags, remove the airway quickly to prevent regurgitation and
possible aspiration of stomach contents.
f. Record Treatment and Evacuate the Patient.
(1)
Complete a Field Medical Card and attach the card to the patient's
clothing.
(2) Evacuate the patient for further evaluation and treatment by a physician.
The patient must be watched constantly so that the airway can be removed in the event
he becomes conscious. During evacuation, check the airway periodically to ensure that
it is free from obstacles and is functioning properly. This is why the oropharyngeal
airway is not recommended in MASCAL and tactical situations when constant airway
monitoring is not possible.
2-5.
COMBI-TUBE AIRWAYS
a. The Combitube (figure 2-9) is an esophageal-tracheal double lumen airway.
It is considered to be an intermediate airway whose abilities lie between the airway
adjuncts oropharyngeal airway (OPA), nasopharyngeal airway (NPA), and an
endotracheal intubation tube (ETT).
b. The Combitube airway is designed to provide a patent airway for a
respiratory/cardiac-arrested patient. The Combitube is a blind-insertion airway device
(BIAD). It has been used successfully in patients with difficult airways secondary to
severe facial burns, trauma, upper airway bleeding, and vomiting where there was an
inability to directly visualize the vocal cords.
MD0542
2-9

 Previous Page
Previous Page
