
(c) If there is no improvement, perform a fluid challenge. Administer
500 cc IV fluid quickly until the patient has received two liters of fluid.
(d) In a hospital setting, if the patient's condition has not improved, an
internal or external pacemaker is considered.
(e) If there is still no improvement, the next step is chest massage.
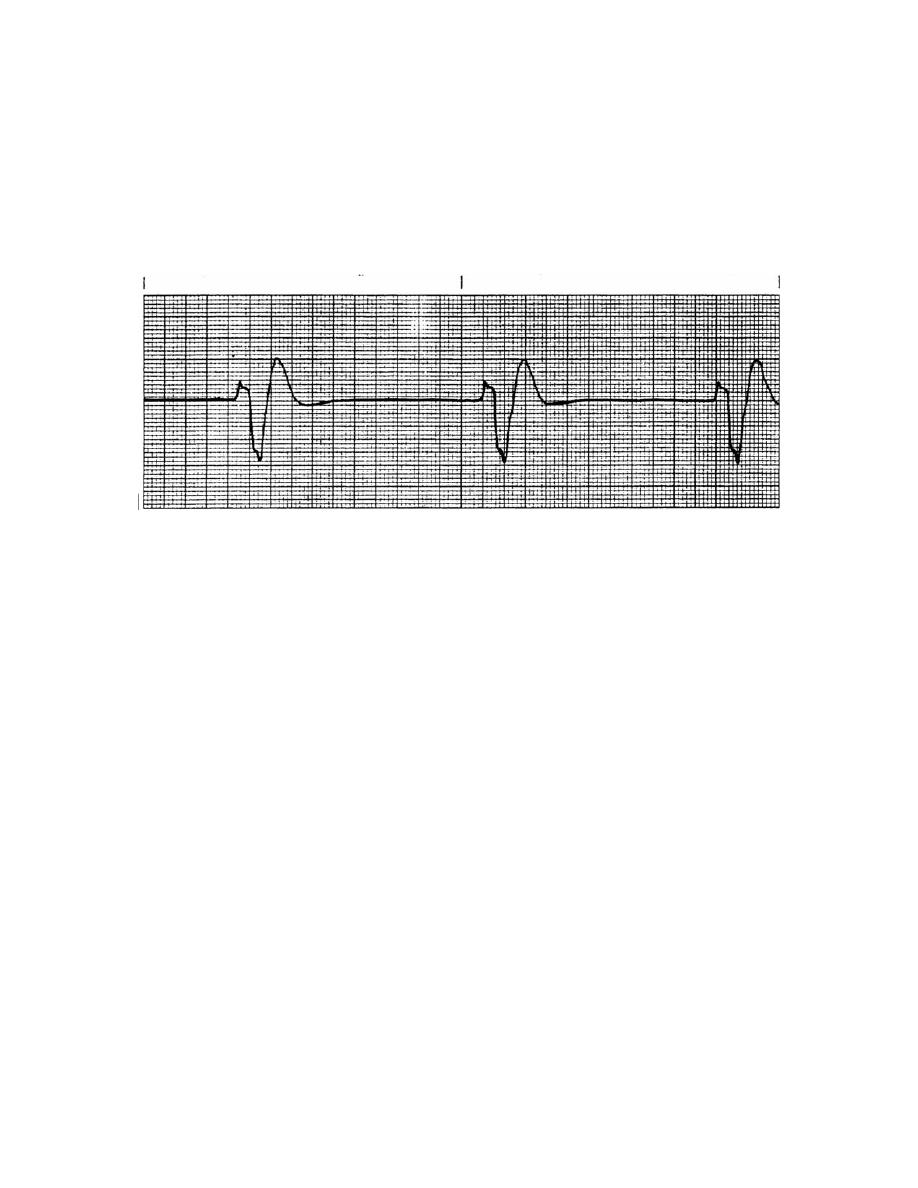
Figure 2-34. Idioventricular rhythm.
2-12. ASYSTOLE (CARDIAC STANDSTILL)
a. Analysis. A straight line on the electrocardiogram indicates an absence of
electrical activity by the heart: no regularity, rate, P waves, P-R interval, or QRS
complex. The casualty is clinically dead. He has no effective cardiac output. Normal
rhythm must be restored within a few minutes by appropriate treatment.
b. Treatment. It is sometimes difficult to distinguish between asystole and
ventricular fibrillation. If there is any doubt, treat the patient for ventricular fibrillation.
When the rhythm is unclear and the possibility of VT exists, defibrillate as for ventricular
fibrillation. If asystole is present, follow this procedure:
(1)
Continue CPR.
(2)
Establish IV access.
(3)
Administer epinephrine, 1:10,000, 0.5 - 1.0 mg IV push.
(4)
Intubate when possible.
(5)
Administer atropine, 1.0 mg IV push, repeated in 5 minutes.
MD0571
2-36

 Previous Page
Previous Page
