
c. The premature infant has a small gastric capacity but a high caloric
requirement. Adequate nutritional support may be achieved by providing frequent
feedings of small amounts using a high calorie formula.
d. The premature infant regurgitates feedings easily because of the poor muscle
tone at the cardiac sphincter. They can only eat small amounts at each feeding. Their
heads should be elevated after eating.
e. In addition to high calorie content, the formula is often supplemented with
calcium, phosphorous, electrolytes (that is, sodium, potassium, and chloride), and
vitamins.
f. When breast milk is required, the mother can pump her breast and the milk
can be fed to the baby at a later time.
g. Inappropriate weight gain of the premature infant in relation to caloric intake
can indicate problems. Usually large weight gain may indicate excessive fluid retention.
No weight gain or a loss may indicate acidosis, sepsis, or malabsorption.
h. The premature infant should be allowed to rest between feedings. The infant
tires easily from procedures and will eat better if rested. Each feedings should not last
longer than 15 minutes.
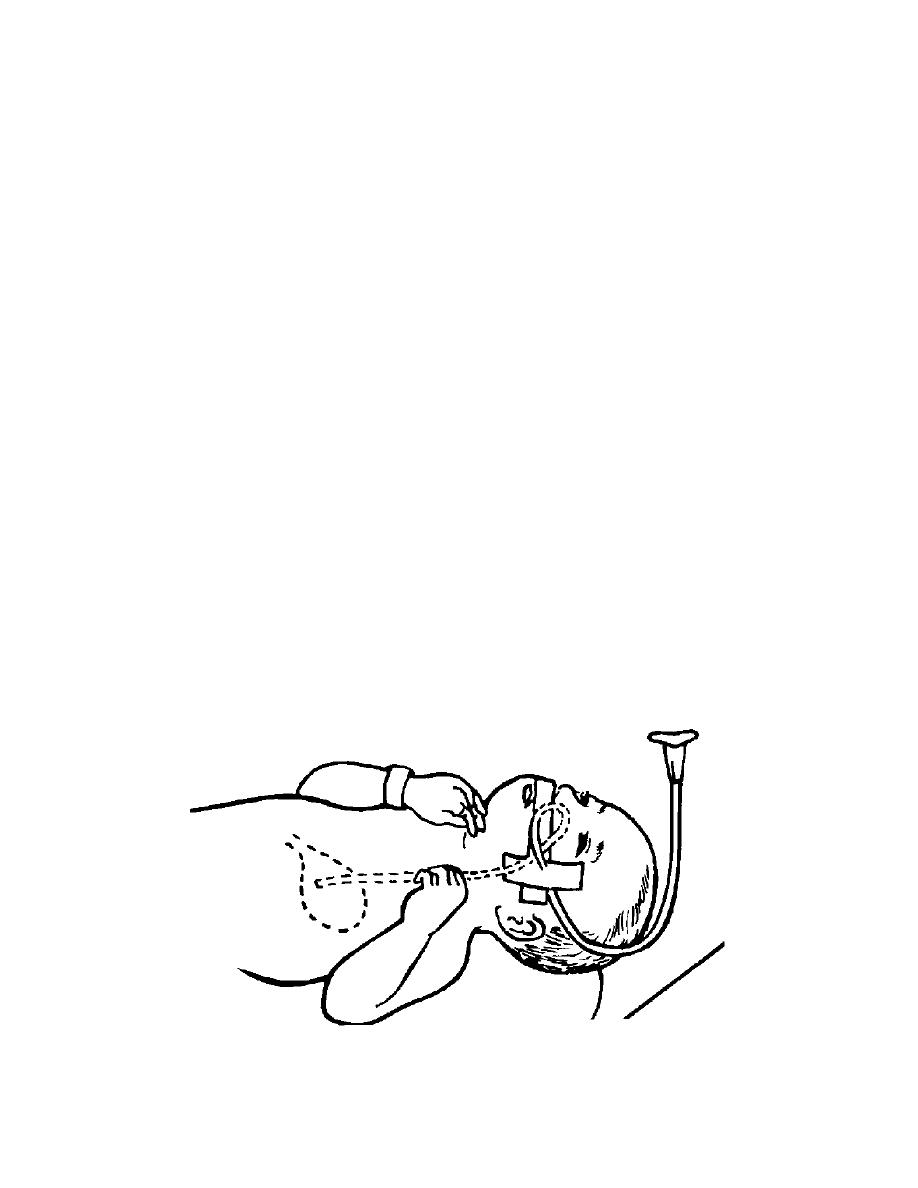
i. Gavage feeding (see figure 10-1) may be required until the preterm infant is
strong enough for the gradual introduction of bottle or breast-feeding. Before each
feeding, stomach secretions are usually aspirated, measured, and the
amount/characteristics are documented. If the infant has more than 2 ml of secretions
in the stomach prior to feeding, he is probably receiving more formula than can be
digested between feedings.
Figure 10-1. Gavage feeding.
MD0922
10-5

 Previous Page
Previous Page
