
(2) This evaluation will help you in identifying the frequency (how often in
minutes contractions occur), intensity (strength of contractions when palpitations are
identified as mild, moderate, or strong [severe]), and duration (how long the contractions
lasts in seconds).
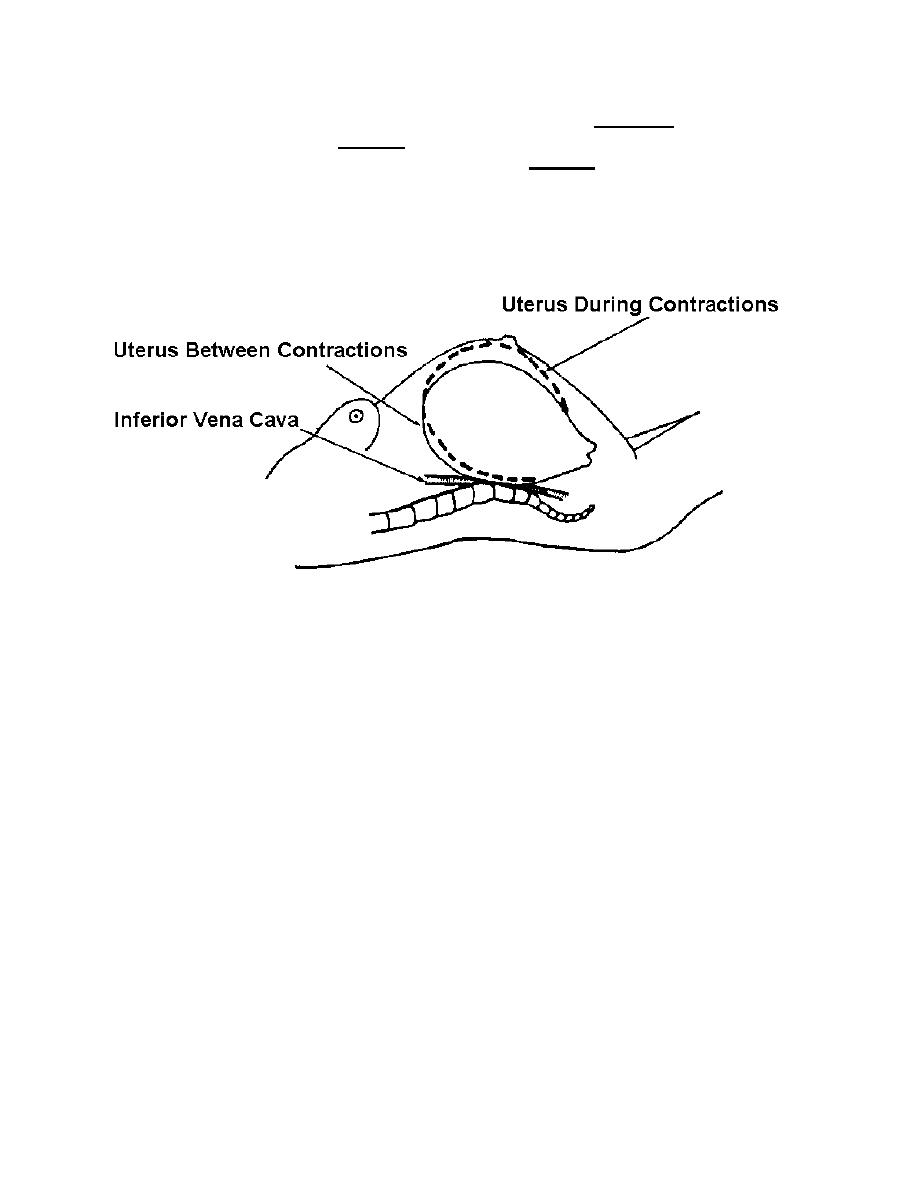
(3) When palpating for contractions, place your hand over the fundal area of
the patient's uterus. Contractions can be felt by your fingers before the patient actually
becomes aware of them. See figure 2-3 for patient experiencing contractions.
Figure 2-3. Uterus between and during contractions.
e. Monitoring and Recording Color and Amount of Show. As labor
progresses, the show becomes more blood-tinged. A sharp increase in the amount of
bloody show coupled with frequent severe contractions may indicate labor is
progressing too rapidly. Report this immediately to the Charge Nurse or physician and
be prepared for possible delivery.
f. Fetal Monitoring.
(1) Fetal monitoring is done to detect presence of fetal life at time of
admission and to detect development of fetal distress during labor. A fetoscope or fetal
monitor may be used to obtain FHTs. Normal fetal heart rate ranges from 120 to 160
beats per minute (BPM). The rate may increase or decrease by 30 BPM during a
contraction. It should return to the baseline immediately after the contraction. A
continued fetal heart rate of greater than or less than 30 BPM from the normal baseline
after contractions may be indicative of fetal distress as defined by:
(a) Fetal tachycardia--FHTs sustained at greater than 160 BPM.
(b) Fetal bradycardia--FHTs sustained at less than 120 BPM.
MD0922
2-10
 Previous Page
Previous Page
